1. Endodontics
High-resolution small field scans are suitable for detecting missed canals, secondary signs of root fracture and perforations
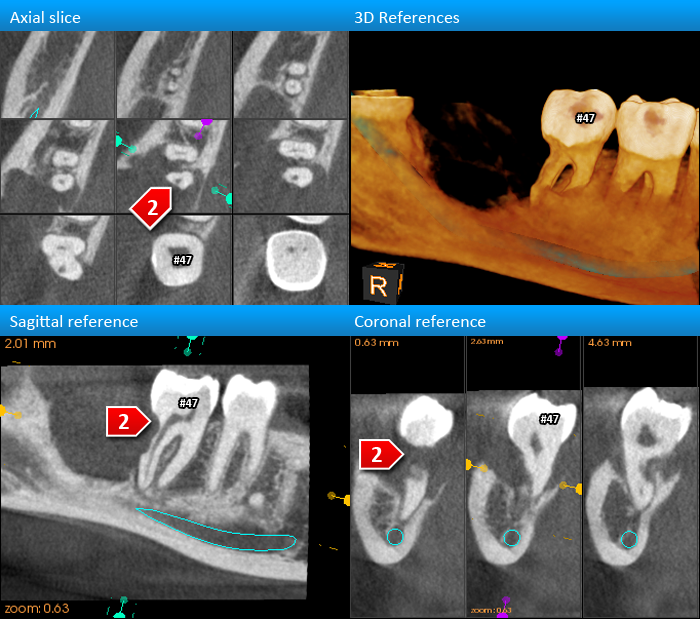
Root perforation
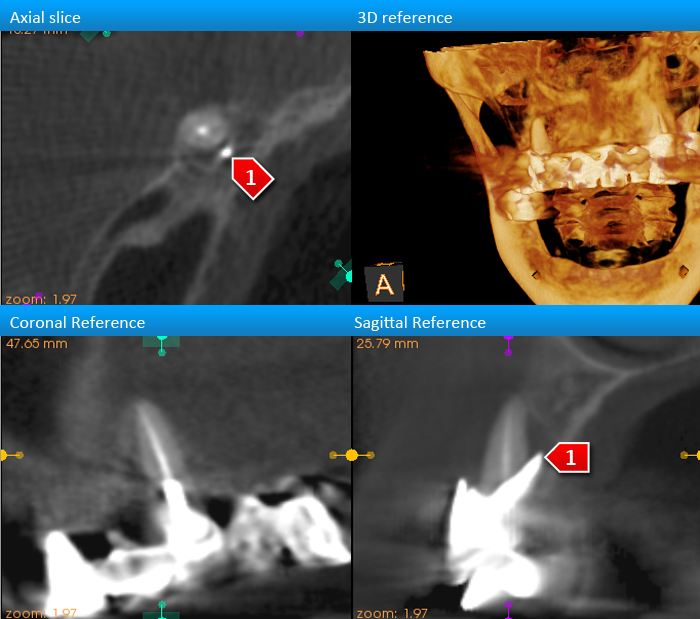
Strongly indicated for the detection of root perforations. A high level of certainty regarding a potential root perforation can be acheived via CBCT. Of course, if a metal post is present in the root canal, image quality will be lower.
Missed Canal
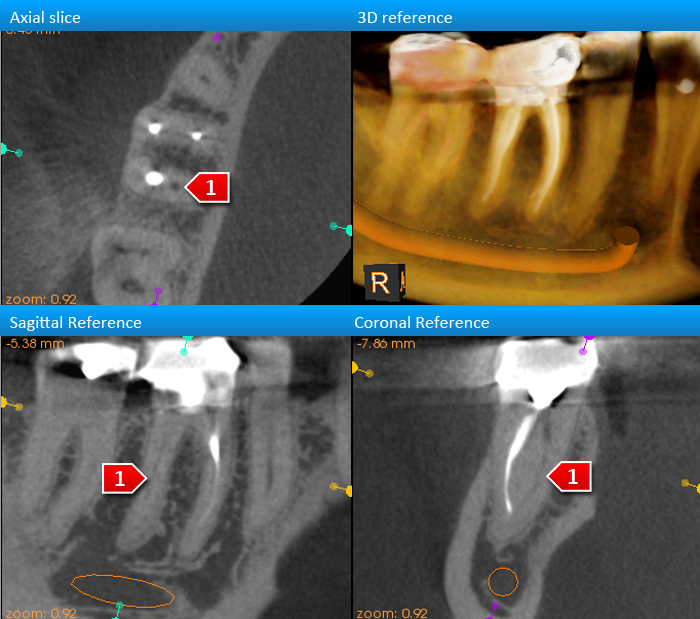
Strongly indicated for the detection of missed canals, primarily by studying the profile (shape) of roots from an axial (occlusal) perspective. You can tell from the root shape whether an additional unfilled canal is present in the mesiobuccal root of maxillary first molars, for example.
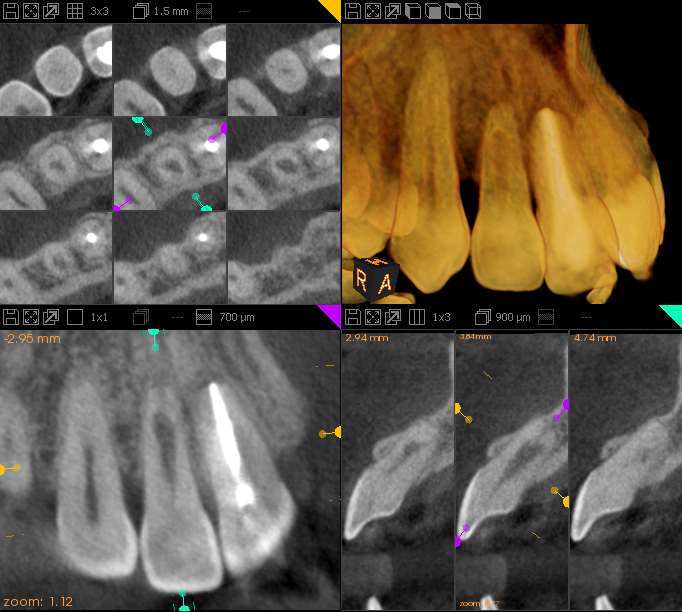
Root fracture (maybe)
Variable results for the detection of non-displaced root fractures. The most reliable radiographic finding is the present of a long narrow pocket along a root surface. Often, beam hardening artifacts can mimic fractures, resulting in an incorrect diagnosis of a fracture where one isn't present.
Occult findings + other
Commonly found during referrals for other indications. This has the potential to alter the treatment plan
2. Root Resorption
Cone beam CT offers an unparalleled means of evaluating internal and external root resorption
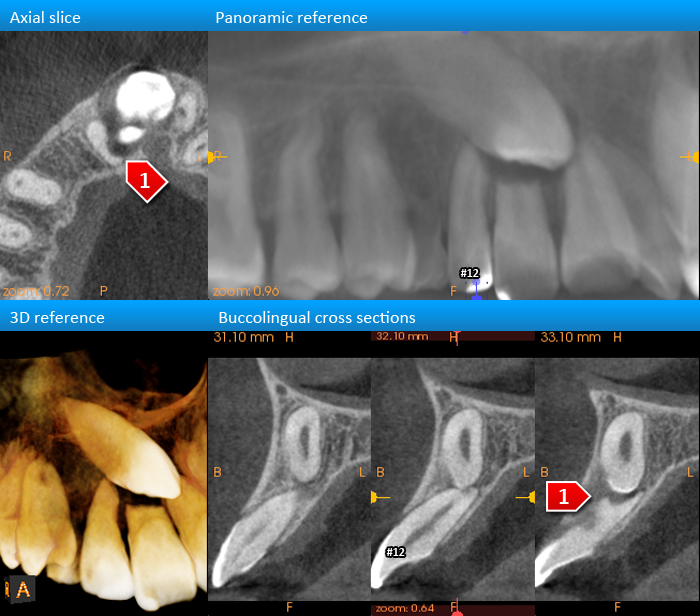
External Resorption
Strongly indicated for the detection of external resorption by adjacent pathologic entities or impacted teeth
Internal resorption
Strongly indicated for the detection of the shape and size of internal resorptive defects in teeth.
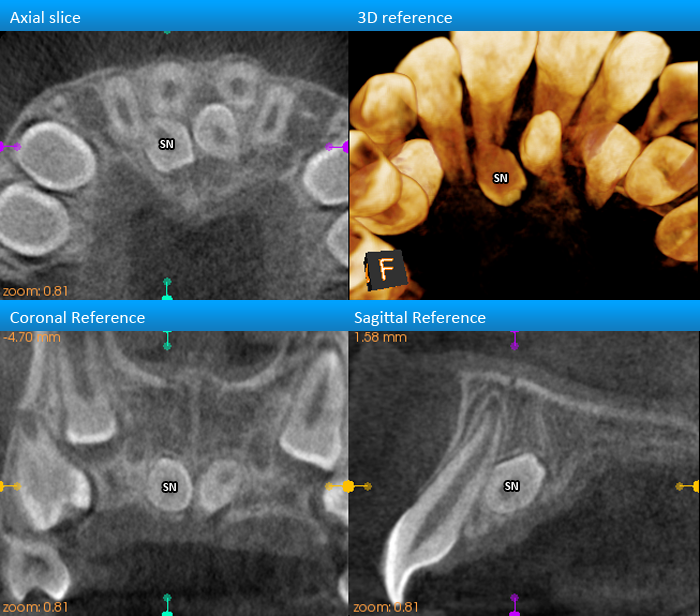
3. Impacted Teeth
CBCT provides a clear visualization of impacted maxillary canines, supernumerary teeth, and wisdom teeth
Orthodontics
Strongly indicated for the localization of impacted maxillary canines and for the evaluation of their effects on the roots of adjacent teeth
Supernumerary Teeth
Strongly indicated for the detection of the position and effects of supernumerary teeth on the surrounding dentition.
Wisdom Teeth
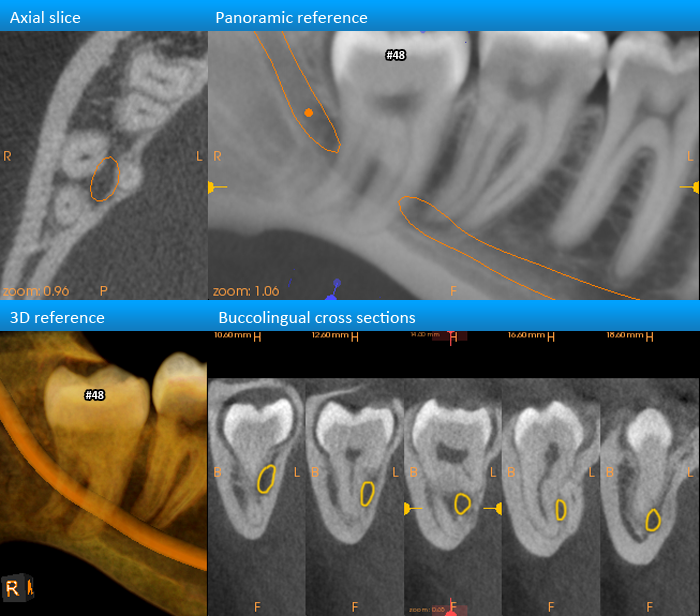
Strongly indicated for the evaluation of the mandibular nerve position and compression level relative to impacted mandibular wisdom teeth.
4. Pathology
The evaluation of the extents of bony pathologic lesions and maxillary sinus lesions are improved with CBCT. Note that soft tissue lesions cannot be effectively assessed (e.g: tongue lesions)
Bone Pathology + trauma
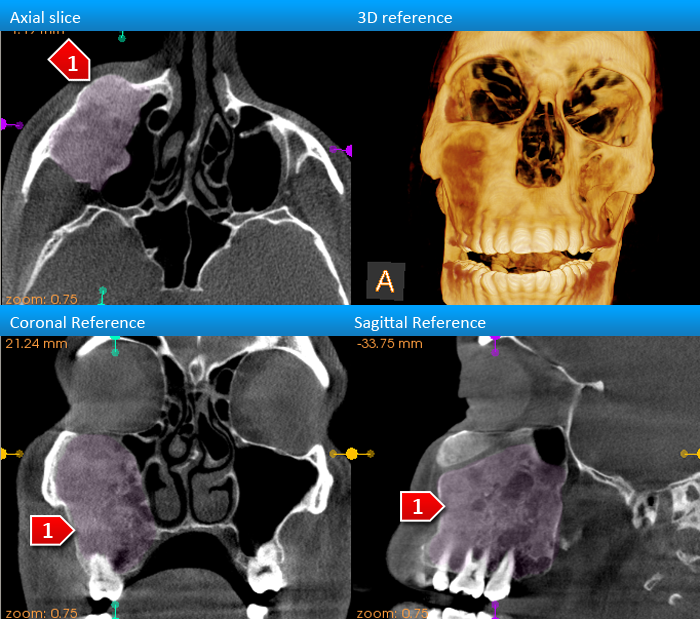
Lesions that are confined to or have an effect on bone can be visualized via CBCT. Often, the extent of the entity and its effects on surrounding structures can be determined, but definitive diagnoses are usually obtained via histopathology.
Maxillary Sinuses
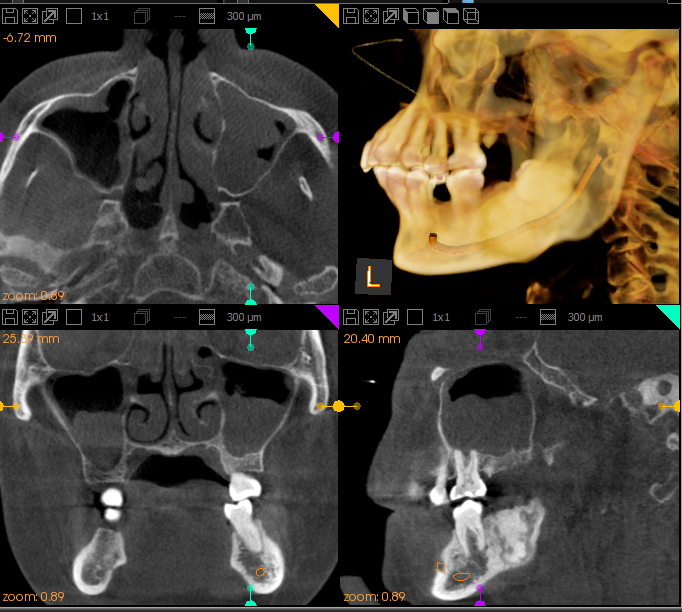
Strongly indicated for pre-surgical evaluation of the maxillary sinuses. The extent and nature of sinus opacification can be deteremined in order to facilitate planning for a sinus lift.
5. Temporomandibular Joint
The TMJs can be evaluated for signs of degenerative joint disease, and when coupled with a clinical exam, can provide an indication of the state of the articular disc
Bones of the TMJ
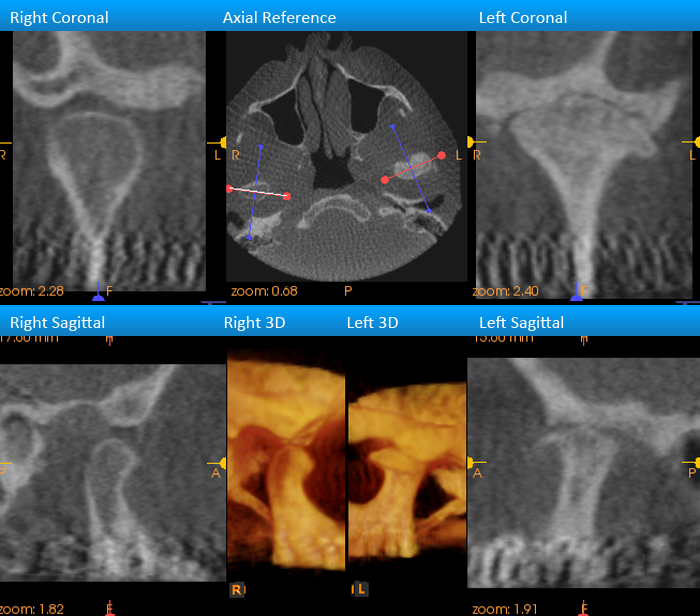
TMJ diseases such as degenerative joint disease can be identified by cone beam CT. However, the articular discs of the joints cannot be visualized directly with CBCT. Disc position must be inferred by the position of the condylar head and by clinical findings. Only an MRI can visualize the discs directly.
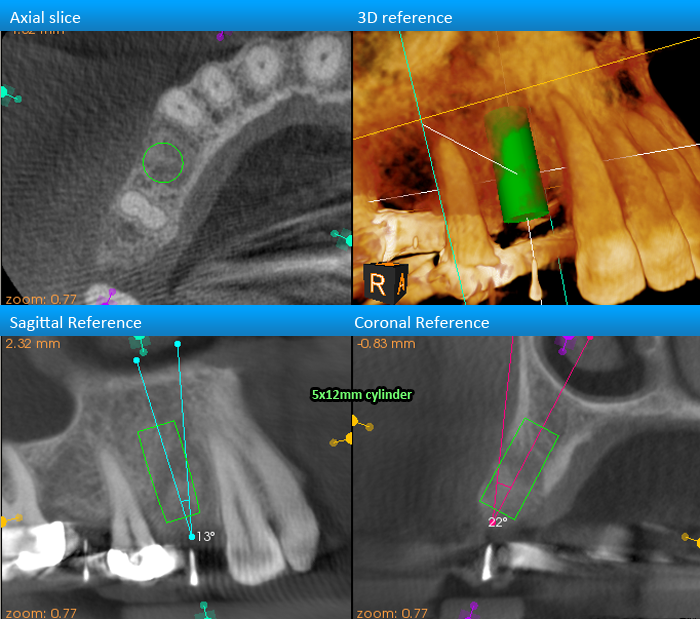
6. Implant Planning
CBCT-guided implant planning can be as involved or as minimal as you want it to be: From bone measurements to CAD/CAM guided surgeries to digital platforms for prosthetically driven planning, and everything in-between.
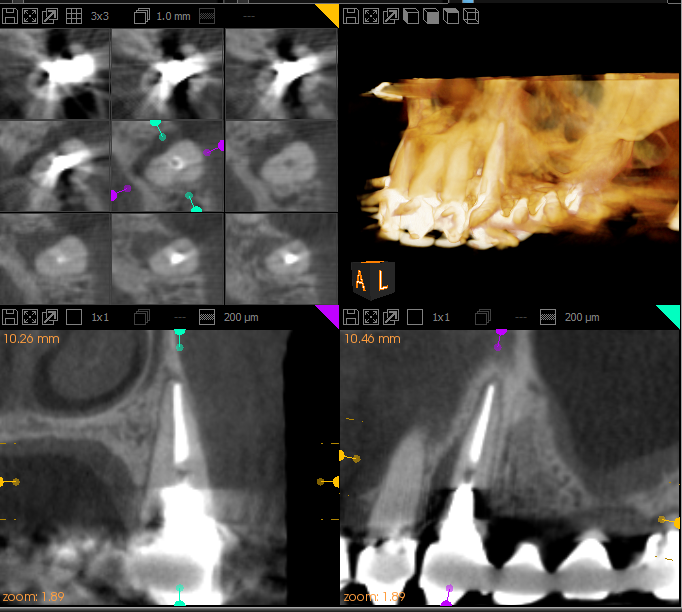
Bone measurements
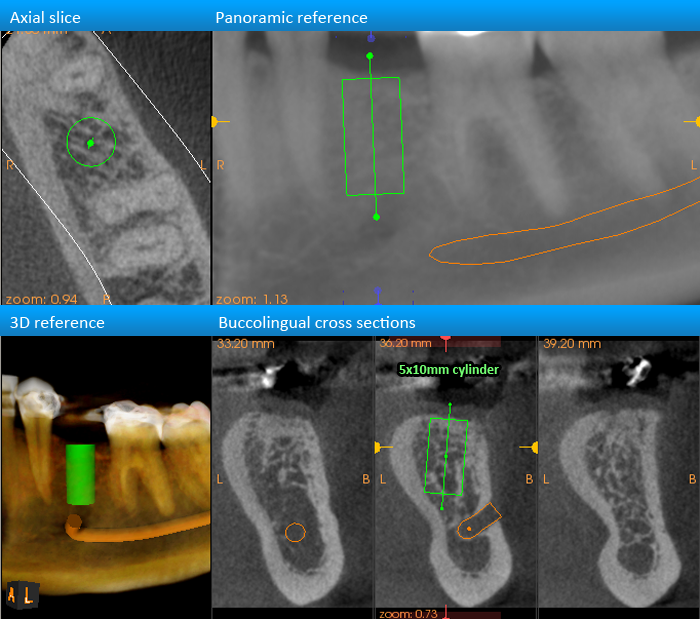
CBCT scans are dimensionally accurate, allowing measurements of bone architecture in putative implant sites to be made.
$150 (1/2 quad) to $295 (4 quad) Measurements 37 Bevel 27 Mx sinus 11 incisive canal IAN Safety zone Free scans
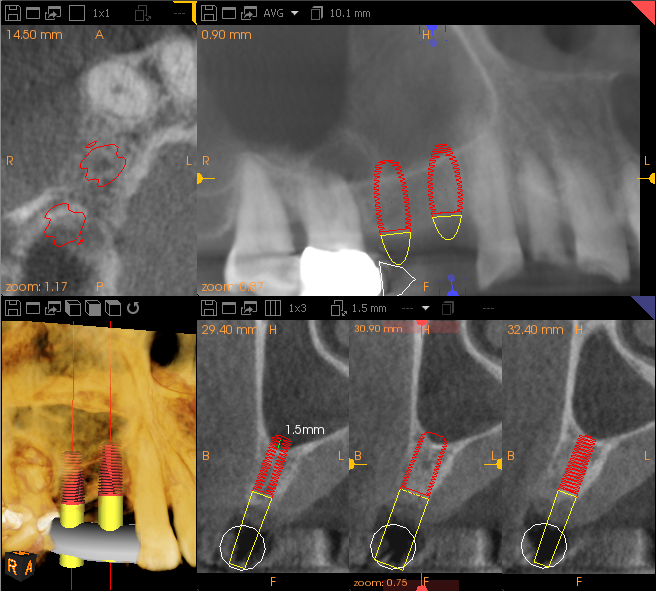
Radiographic guides
Dental labs can fabricate radiographic guides that can serve as an indicator for potential implant orientations. After the scan, the guide can be modified to provide surgical guidance during implant placement.
Accuplant + CoDiagnostix
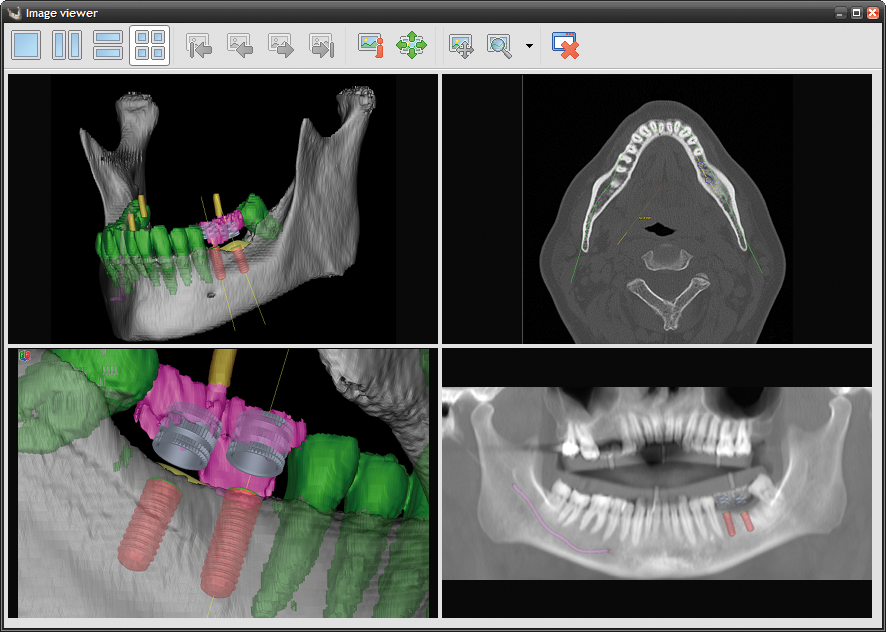
Tooth-supported guides based on computer assisted planning can be fabricated in-house by a lab with the CoDiagnostix system. This guide is preferred for tooth supported cases at Canaray because it can be reliably seated with little to no adjustment. The most economical system for computer-guided surgery.
Simplant

Mucosa and Bone-supported guides based on computer assisted planning are fabricated in Materialise's centralized facility in the USA. This system is preferred for mucosa or bone-supported guides because a bone-supported guide can be fabricated without an impression of the bone. Software conversions are required.
NobelGuide
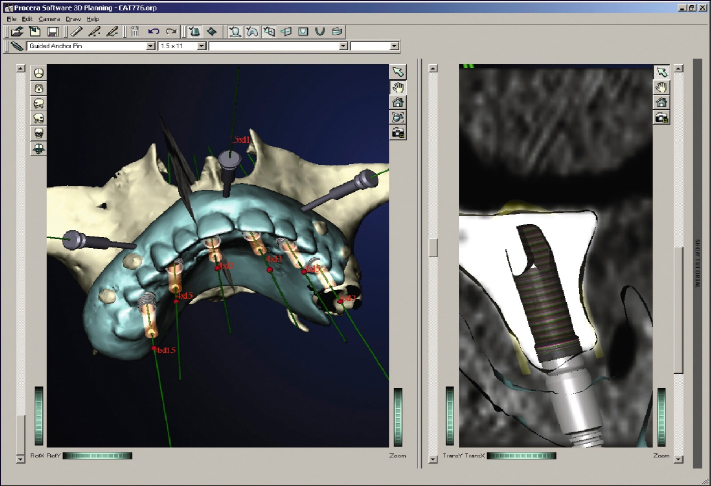
For Nobel implants only. A specially constructed radiographic guide is necessary to use this system. The clinician receives the scan data and plans the case independently.
Other systems

New systems for CT-guided imaging are constantly emerging. If your system is not on this list, contact us at 1-877-498-9279 and we'll see what we can do to accommodate your needs.